Adolescent Violence: A veiled threat to HIV epidemic control.
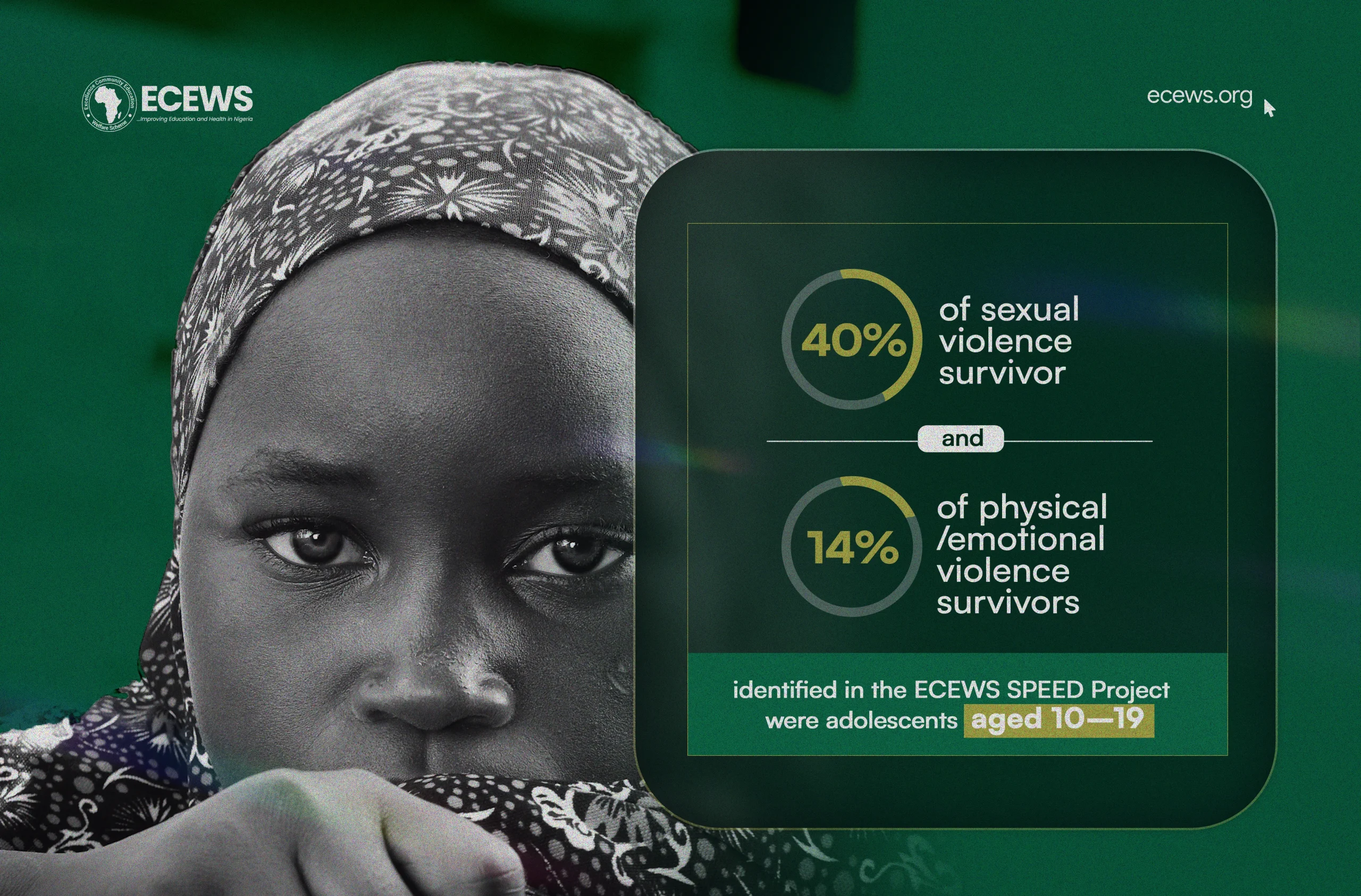
Violence against adolescents with HIV results in trauma, deterrence in ART adherence and epidemic control. Within the ECEWS SPEED project, adolescents aged 10–19 accounted for 40% of the 1,412 identified sexual violence survivors. Violence has profound implications for HIV epidemic control. For adolescent teens already a vulnerable fraction of the population in the HIV response, exposure to violence creates major barriers across the entire HIV cascade. Addressing adolescent violence is essential to improving HIV control in teens and breaking down these critical barriers.
Forms of Violence and Their Impact on the HIV Cascade
Sexual Violence: Sexual violence affects the HIV cascade in the following ways:
Physical Violence: This remains the most visible form of violence affecting adolescents.
Emotional and Psychological Violence: Though less visible, emotional violence, including verbal abuse, humiliation, isolation, intimidation, psychological manipulation, and deliberate attempts to undermine an adolescent’s self-esteem and mental health, can be equally damaging.
Technology-Based Violence: Approximately 15% of adolescents (around one in six) experience cyberbullying, according to recent WHO data. Technology-based violence also includes online sexual exploitation, sextortion, non-consensual sharing of intimate images (revenge porn), online grooming by predators, and exposure to violent or traumatic content.
Economic Violence: Though less commonly discussed, it significantly impacts adolescents, particularly in contexts of intimate partner relationships and family dynamics. Adolescents in vulnerable households are often denied resources, forced into exploitative labor, or coerced into transactional sex to survive. Child marriage, which affects 43% of girls in Nigeria before age 18 (UNICEF, 2020), is another form of economic and structural violence that perpetuates poverty and poor health outcomes.
Peer-to-Peer Violence: This encompasses a broad spectrum of harmful behaviors that occur between adolescents, including bullying, fighting, gang violence, dating violence, peer pressure, and various forms of harassment, which all significantly impact adolescents.
Factors that enable violence
Understanding violence among adolescents requires examining the interplay of individual, relationship, community, and societal factors that contribute to both perpetration and victimization.
Individual factors include a history of abuse, mental health conditions, substance abuse, impulsiveness/poor emotional regulation, and a lack of conflict resolution skills. Adolescent brain development, particularly the ongoing maturation of the prefrontal cortex responsible for impulse control and decision-making, contributes to heightened risk-taking and reactive behaviors.
Family and relationship factors play a crucial role, including exposure to domestic violence, lack of parental supervision or involvement, and poor parent-child communication.
Community and environmental factors include poverty, lack of access to quality education, lack of positive role models, and community norms that tolerate violence.
Societal factors encompass media violence, non-implementation of policies and laws to protect youth, and insufficient investment in prevention and intervention programs.
Consequences of Violence
Apart from affecting HIV epidemic control, violence also has the following consequences:
Increased risk of other STIs and unintended pregnancies, poor mental health outcomes, including depression, anxiety, and suicidal tendencies, post-traumatic stress disorder, substance abuse, Injuries, disability, perpetuation of the cycle of violence, as survivors may later become perpetrators, reduced productivity, poor academic outcomes, and early dropout.
Strategies for improvement
Interventions for Victims of Violence
For adolescents who have experienced violence, targeted interventions include;
Unless violence is addressed systematically, gains in epidemic control will be undermined. Protecting adolescents from violence safeguards not only their health and rights but also the future of HIV prevention, treatment, and epidemic control.
Rosemund Onuoha is a public health professional whose areas of expertise include violence prevention and child protection. She supports the integration of survivor-centered responses within ECEWS’s CDC-funded SPEED Project, championing equity and improved well-being for vulnerable populations.